
Lisbon to Me
Despite my aggressively Irish name, my grandmother is 100% Portuguese, so I know a thing or two about Catholic Portuguese queens. Perhaps that’s why I felt particularly sensitive to the tragic demise of Maria when Stefanie introduced me to her story. Maria’s story is the perfect confection of many of the themes we have explored in previous series; the delineation between normal grieving and mental illness; the dangers of inbreeding; the link between infections (in this case measles) and the manifestation of psychiatric symptoms. If you are interested in those topics, I recommend you go back and check out our series that cover them! But today, I want to focus on a topic that was near and dear to Maria and has become the center of modern discussions surrounding her mental health: religion.
When Saul Became Paul
Musings on the neurobiological origins of religious experience began as far back as Hippocrates, and have focused largely on one disease: epilepsy. In 1987, an article was published in Journal of Neurology offering a provocative retrospective diagnosis for Saint Paul, a prominent figure in the New Testament Bible. Saint Paul persecuted followers of Jesus until he experienced a sudden loss of vision and heard the voice of Jesus telling Paul to stop persecuting him and to go seek out one of his disciples. Paul went on to become the most important evangelizer of the early church. The paper argues that Paul’s spiritual experience was actually consistent with temporal lobe epilepsy, which is a type of seizure localized to the part of the brain important for memory formation and auditory processing.

And indeed, seizures can often cause visions or other sensory experiences of a religious nature. As we discussed in a previous series, seizures happen when particular regions of the brain have disrupted patterns of electrical signaling. Depending on where the seizure happens, a person could have visual, auditory, motor, or emotional experiences. And interestingly, these sensory experiences can have religious themes, like hearing the voice of God or seeing angels. Studies have found that around 3% of epilepsy patients have religious experiences during, after, or between seizures, with most of these patients having the same temporal lobe epilepsy that has been attributed to Saint Paul.
Russian author Fyodor Dostoyevsky was an epileptic whose seizures had an intense spiritual character. Ever the wordsmith, he wrote about these experiences: “The air was filled with a big noise, and I thought that it had engulfed me. I have really touched God. He came into me myself, yes, God exists, I cried, and I don’t remember anything else. You all, healthy people can’t imagine the happiness which we epileptics feel during the second before our attack. I don’t know if this felicity lasts for seconds, hours, or months, but believe me, for all the joys that life may bring, I would not exchange this one.”
Soul Responsibility
The connection between spirituality and epilepsy has, frankly, been lazily exploited to support the position that religion is a delusion. But clearly not everyone who is religious has seizures, or even has sensory encounters with the divine. In a remarkably balanced review by Orrin Devinsky and George Lai from New York University, the research on epilepsy and religious experiences is synthesized to come to the simple but profound conclusion that there is a neurological basis for religion, not that religion is a symptom of neurological illness. Moreover, Devinsky and Lai point out that religiosity in epileptic patients could alternatively be explained as a reaction to the suffering and isolation caused by their disease; a longing for comfort and meaning.
A change in a person’s religious beliefs as a human reaction to suffering and trauma is a hypothesis that is too often neglected in neuroscience research on spirituality. A study published in June from a group at Harvard looked at patients who reported changes in religiosity following neurosurgery or brain damage. By looking at changes in brain connectivity between the lesioned area of the brain and other regions using MRI, the authors identified the periaqueductal gray matter (PAG) as a region associated with changes in religiosity ratings. The PAG is a brain region that plays important roles in “fear conditioning, pain modulation, and altruistic behavior.” They also point out that this brain circuit is associated with delusions and alien limb syndrome, when someone feels as though one of their extremities is being controlled by someone else.

In the discussion section they stress that, “our results do not imply that religion is a delusion”, but unfortunately that caveat is not included in the abstract (the short summary that is often the only part of an academic paper that people bother to read). In addition, they fail to consider that a change in self-reported ratings of religiosity could be human reactions to the major life events of having a brain tumor or experiencing traumatic brain injury in the Vietnam War (the two patient populations studied in the paper). I am not arguing that religion should be off-limits to neuroscientific research. However, I would urge neuroscientists to approach the topic with sensitivity and an openness to the possibility that not everything can be explained by biology.
This has all been a very long way to say that studying religion through a neuroscientific lens is a delicate thing. And as we look at Maria, I want to avoid giving the impression that her religious inclinations were a result of her mental illness. Given how devout she was from her youth, I think it’s more likely that her mental illness distorted her relationship with her faith, making it a source of torment.
The line between religious fervor and religious mania is thin and, understandably, a sensitive area of debate. As a practicing Catholic and neuroscientist, I appreciate how important it is to respect religious beliefs while at the same time acknowledging that they can be distorted and contribute to mental illness.
But a problem arises in studying religious mania: who gets to decide what is normal and what is not? Were saints who had visions actually just mentally ill? Are religious communities who practice strict self-denial and even physical penances insane? If you ask my siblings, should I be seeing a therapist because I go to church multiple times a week? This brings up an issue that Stefanie and I have addressed many times on the blog: normal and abnormal are, to some extent, constructs of society. So where does that leave neuroscientists in the quest to understand the biological basis of religion?
Jesus, Take the Wheel
The consensus among medical historians is that Maria (and all of her sisters) suffered from diseases in the major depressive disorder family. This diagnosis explains Maria’s more dramatic symptoms, like the meltdowns she experienced that left her unable to talk or function. But since we previously covered the neurobiology of depression in our Juana series, I want to stick with our theme and zero in on Maria’s unhealthy relationship with religion during her battle with mental illness.
Even before Maria’s mental decline, she had a more fire and brimstone view of God than many Christians do today. Stefanie told us last week that she interpreted tragedies like a devastating earthquake as divine punishment for human sin. After her mental illness emerged, Maria became fixated on the possibility of her damnation and distressed by thoughts of her faith. Her anxiety about the fate of her soul seemed to be a key driver of her depressed mood.
More than your average Catholic guilt, this kind of obsession with the state of one’s soul is known as scrupulosity. According to the National Catholic Register, scrupulosity “involves excessive anxiety about the sinfulness of particular actions.” People struggling with scrupulosity often reconfess the same specific sins, doubting that they can be forgiven, and believe that they have committed mortal sin where none was committed. But scrupulosity isn’t found just within the Catholic church, or within religious institutions in general. Scrupulosity is actually just one form of the better known disease obsessive compulsive disorder (OCD).
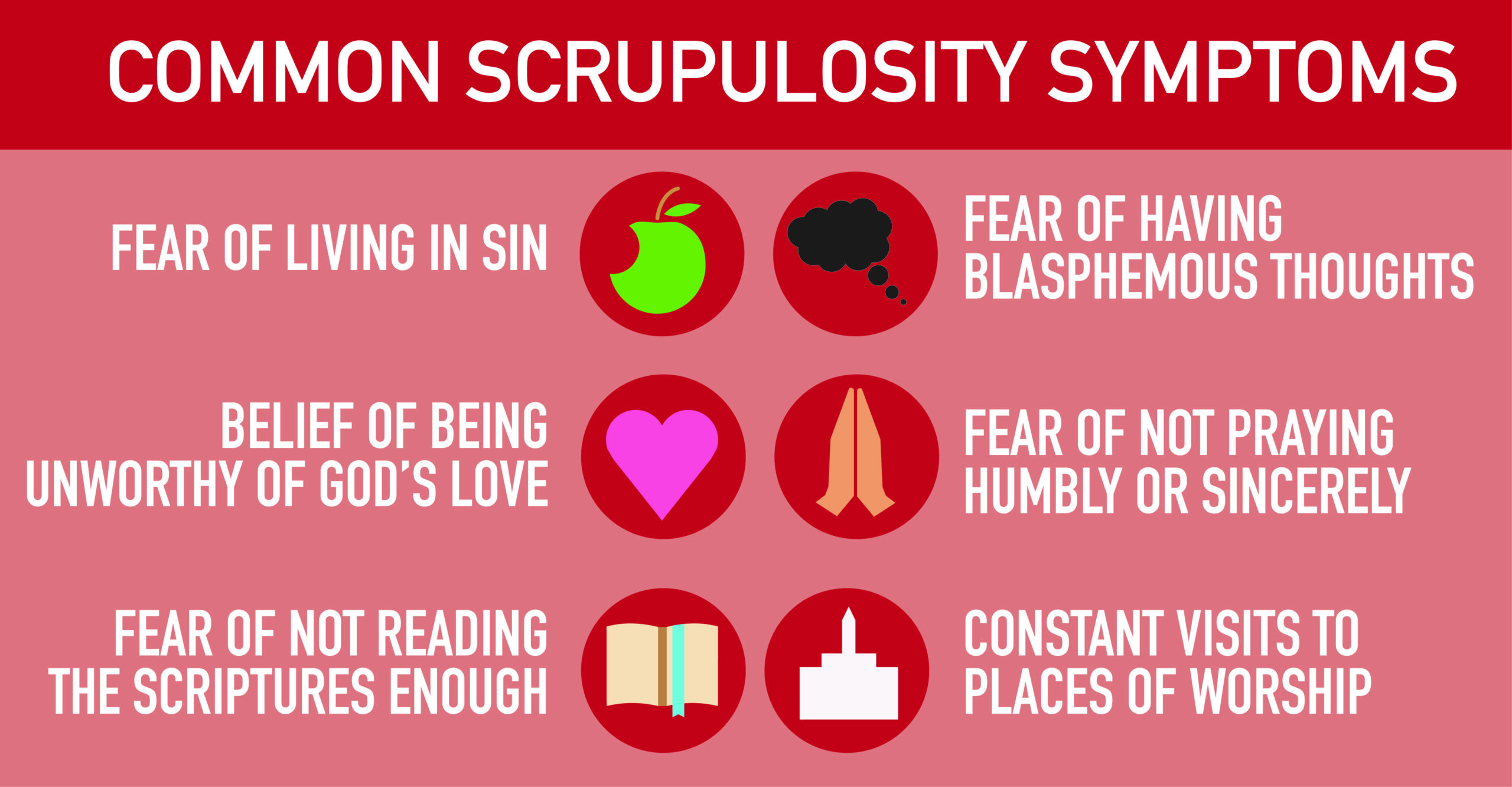
OCD is more than liking a color coded calendar or spotless kitchen. People with OCD are assailed with an obsessive, unwanted, unpleasant thought. This repetitive thought pattern causes anxiety that can only be relieved by performing certain actions, called compulsions. The obsessive thoughts in cases of scrupulosity usually focus on damnation and sin, and the accompanying compulsions can be praying, reciting scripture, going to confession, or taking on penances.
Vicious Cycle
A 2019 paper from researchers at the University of Michigan nicely showed neurobiological underpinnings of this disease by comparing MRIs from OCD patients to those of healthy controls. The researchers analyzed results from many previously published studies in which participants performed specific motor tasks that measure something called inhibitory control. In these tasks, participants have to ignore certain stimuli in order to perform a certain action or to stop an action that was already initiated when they see a stop signal. When people made an error on the task, the brain would send a signal to try to correct the motor output. But in OCD patients, the brain network that received this signal didn’t really listen, so the error message became stronger. The overactivity of the error signaling ended up backfiring by making the person more anxious, causing more mistakes, which in turn amplified the error signal even more.
These results aligned with previous studies that found altered activity in OCD patients in circuits responsible for error processing and inhibitory control. The neural response to errors in these tasks also mirrors the psychiatric symptoms of OCD. Basically, compulsive behaviors trigger an error signal of sorts because these behaviors are often at odds with a person’s goal (think: someone with OCD who compulsively washes their hands but is trying to decorate a cake). However, this error signal is unable to suppress the impulsive behavior and only serves to increase anxiety, leading to more compulsive behavior (for example, because I can’t stop washing my hands, it must be important to be washing my hands).

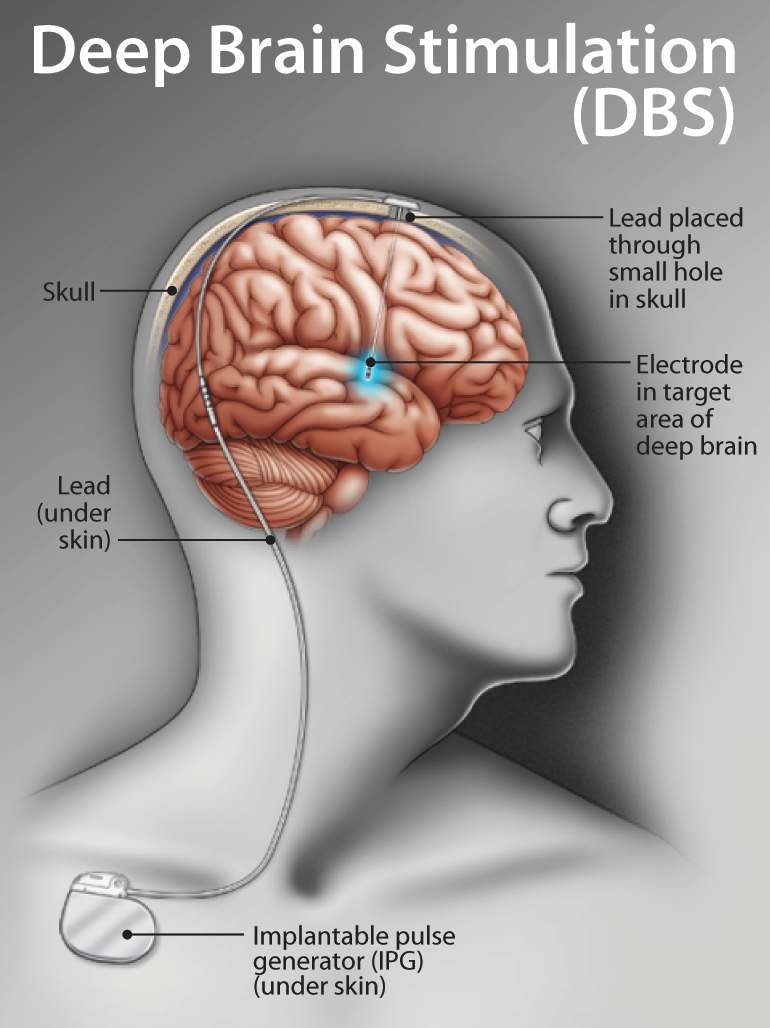
Correcting this impaired neural communication is the target of experimental therapies for OCD. Deep brain stimulation (DBS) is a therapy for movement disorders in which an electrode is placed in a target region of the brain to control neural signaling. Think of it like a pacemaker in your brain. DBS has also been explored in the most severe cases of OCD that don’t respond to treatment. Starting in the 1950s, doctors found success in treating OCD patients by performing surgeries in which they damage part of the brain called the cortico-striato-thalamo-cortical circuit (CSTC), which overlaps with the regions of altered signaling identified in the MRI study I mentioned earlier. Surgeons realized that by using DBS, they could control the signaling of the CSTC rather than destroy it, leading to more personalized care. DBS for OCD is still exploratory, and given the few number of patients who would be eligible for an experimental surgery, we are still some years away from a consensus on its use. But as more is understood about the altered communication patterns in the brains of OCD patients, we are inching closer to being able to treat people with this debilitating disease.
Spiritual Warfare
Science and religion are often pitted against one another, but the case of Maria I of Portugal highlights how intertwined they really are. Her faith was always an important part of her life, but her struggles with depressive disorders and what I believe was likely OCD took what should have been a source of peace and strength and turned it into her personal hell. We are used to hearing about how disputes over religion changed the course of history, but while Maria’s spiritual warfare was going on inside her mind, it had no less of an effect on the future of Portugal. And as a result, Brazil. Come back next week when Stefanie tells us how.
References
Akin, J. (2014, June 31). 6 Tools for the Scrupulous. Retrieved from https://www.ncregister.com/blog/6-tools-for-the-scrupulous
Devinsky, O., & Lai, G. (2008). Spirituality and Religion in Epilepsy. Epilepsy & Behavior,12(4), 636-643. doi:10.1016/j.yebeh.2007.11.011
Ferguson, M. A., Schaper, F. L., Cohen, A., Siddiqi, S., Merrill, S. M., Nielsen, J. A., . . . Fox, M. D. (2021). A neural circuit for spirituality and religiosity derived from patients with brain lesions. Biological Psychiatry. doi:10.1016/j.biopsych.2021.06.016
Kahn, L., Sutton, B., Winston, H. R., Abosch, A., Thompson, J. A., & Davis, R. A. (2021). Deep Brain Stimulation for Obsessive-Compulsive Disorder: Real World Experience Post-FDA-Humanitarian Use Device Approval. Frontiers in Psychiatry,12. doi:10.3389/fpsyt.2021.568932
Landsborough, D. (1987). St Paul and temporal lobe epilepsy. Journal of Neurology, Neurosurgery & Psychiatry,50(6), 659-664. doi:10.1136/jnnp.50.6.659
Norman, L. J., Taylor, S. F., Liu, Y., Radua, J., Chye, Y., Wit, S. J., . . . Fitzgerald, K. (2019). Error Processing and Inhibitory Control in Obsessive-Compulsive Disorder: A Meta-analysis Using Statistical Parametric Maps. Biological Psychiatry,85(9), 713-725. doi:10.1016/j.biopsych.2018.11.010
Peters, T. J., & Willis, C. (2013). Mental health issues of Maria I of Portugal and her sisters: The contributions of the Willis family to the development of psychiatry. History of Psychiatry,24(3), 292-307. doi:10.1177/0957154×13482832
Pollard, A. (2010). Scrupulosity. Retrieved from https://iocdf.org/wp-content/uploads/2014/10/IOCDF-Scrupulosity-Fact-Sheet.pdf

One thought on “Living on a Prayer”