
Diana In Her Own Words
In past series here on ULTC, I have had to rely on historical documents and secondhand sources to piece together the inner workings of our subjects’ minds. But this month, I don’t have to formulate an armchair diagnosis or scour JSTOR; I can go straight to the source. Princess Diana is the most modern royal we have covered on the blog, but she’s also the most accessible. As a result, we have her own words about her battles with mental illness, words that shattered the “keep calm and carry on” tradition of the British monarchy and forever changed the way people think and talk about mental health.

Although Diana’s experiences with mental illness were covered in the 1992 biography by Andrew Morton, she had to deny her involvement in the project because of her royal status. So, the first time Diana publicly talked about her mental health was in her 1995 BBC tell-all interview with Martin Bashir. Breaking royal protocol, she aired the dirty laundry of her failing marriage with Prince Charles and the psychological effects of life in the royal family. As Stefanie told you last week, the BBC reopened an investigation into Bashir in December 2020 over allegations that he coerced Diana into the interview by forging documents suggesting that the Queen had hired people to spy on her. Even so, the contents of the interview remain achingly relatable to anyone who has suffered from mental illness. Her words will serve as guideposts as we explore the neurobiology behind what she suffered.
“I was crying out for help, but giving the wrong signals, and people…decided that was the problem – Diana was unstable.” What were these signals, and what do they reveal about the royal who changed the monarchy forever?
A Secret Disease
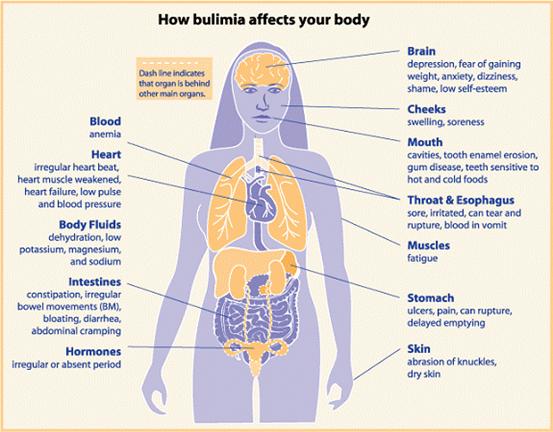
“I had bulimia for a number of years. And that’s like a secret disease. You inflict it upon yourself because your self-esteem is at a low ebb, and you don’t think you’re worthy or valuable. You fill your stomach up four or five times a day – some do it more – and it gives you a feeling of comfort. It’s like having a pair of arms around you, but it’s…temporary. Then you’re disgusted at the bloatedness of your stomach, and then you bring it all up again. And it’s a repetitive pattern which is very destructive to yourself… it was my escape mechanism, and it worked for me, at that time.”
First we should distinguish between bulimia and anorexia, the two most well known eating disorders. The latest edition of the DSM outlines the diagnostic criteria for anorexia as restricted food intake leading to “significantly low body weight in the context of age, sex, developmental trajectory, and physical health”, fear of gaining weight, and “disturbance in the way in which one’s body weight or shape is experienced, undue influence of body weight or shape on self-evaluation, or persistent lack of recognition of the seriousness of the current low body weight.” Anorexia can further be categorized as a restrictive type, in which food intake or excessive exercise leads to weight loss, or binge/purge type, in which patients binge eat or use laxatives, self-induced vomiting, or diet pills to lose weight. In contrast, a bulimia diagnosis requires the occurrence of weekly binge eating episodes followed by behaviors to offset weight gain, similar to the binge/purge subtype of anorexia that I mentioned before, for at least 3 months. The difference here is that people suffering from bulimia are not restricting their food intake and therefore do not show the drastic weight loss characteristic of anorexia. As Diana noted in her interview with Bashir, “the thing about bulimia is your weight always stays the same, whereas with anorexia you visibly shrink. So you can pretend the whole way through. There’s no proof.”
However, despite the differences between anorexia and bulimia, clinical data suggests that they are related. 25-30% of people diagnosed with bulimia previously were diagnosed with anorexia. In addition, anorexia and bulimia have shared genetic risk factors, explaining why both disorders are transmitted within families. This is consistent with the fact that Diana’s older sister, Sarah, struggled with anorexia.
Both Diana and Sarah’s eating disorders emerged during their teen years, which is a defining feature of eating disorders. According to Diana, her battle with bulimia started shortly after she began dating Prince Charles and he made an offhand comment calling her “chubby”. This highlights the complicated etiology of eating disorders. If you think back to your middle and high school days, I am sure you remember the heightened self consciousness and desire to fit in and be liked that you experienced with the onslaught of pubertal hormones. These social factors are certainly an important factor in the onset of bulimia and anorexia. However, as I mentioned before, there are also genetic factors at play, shattering the misconception of eating disorders as vain attempts to achieve societal beauty norms. Think of similar dynamics we have talked about before on the blog: an environmental or social trigger setting off a genetic predisposition. In this case, that trigger was Prince Charles’ inserting his foot in his mouth and commenting on the figure of his teenage bride-to-be.
To a large extent, the neurobiology of eating disorders remains a black box. Anorexia and bulimia are far more prevalent in women, and onset coincides with puberty, so there could be a hormonal driver. Eating disorders often emerge after a period of decreased food intake, so could be related to the physiological effects of acute malnutrition. But because the dominant symptom of bulimia is binge eating, researchers have long been interested in whether patients have alterations in the signals that control eating and satiety.
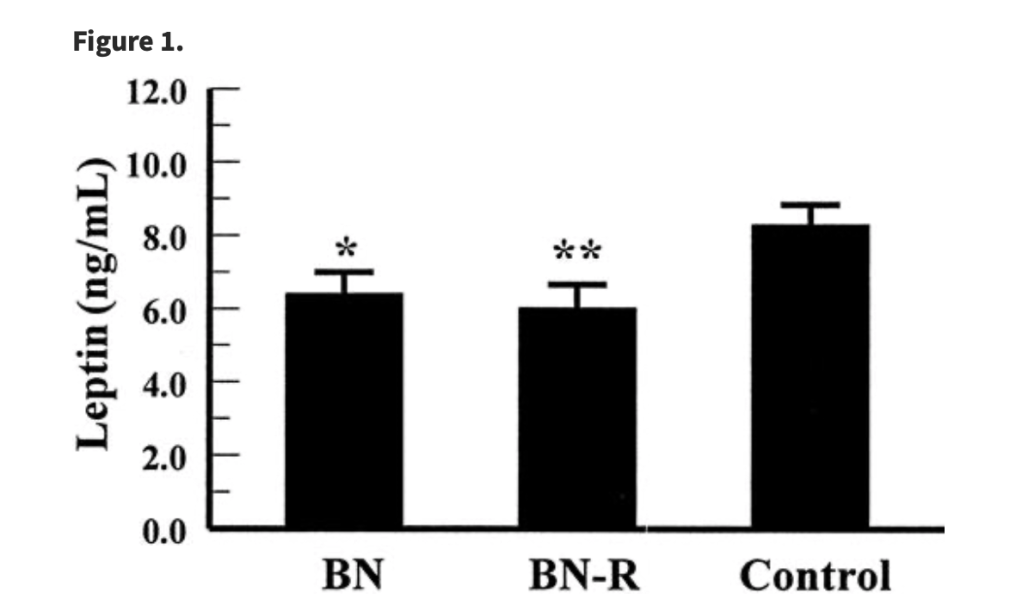
One of these signals is called leptin. Leptin is expressed in fat tissue throughout the body and its levels fluctuate depending on the amount of energy stores available. Leptin can bind to receptors of neurons located in an area called the arcuate nucleus of the hypothalamus in the brain. Once bound, leptin can activate neurons that produce anorexigenic signals, or those that tell the body you aren’t hungry, and suppress neurons that produce orexigenic signals, the ones that tell you it’s time to eat. The overall effect is that appetite is suppressed. A landmark 2000 paper from a team at Harvard Medical School found that leptin levels were lower in women with bulimia than in female controls. This could explain why people with bulimia are less likely to feel full or satisfied after eating, making them more likely to engage in binge eating behaviors. Leptin is also involved in the regulation of many neuroendocrines, hormones that act in the brain, that are similarly involved in the maintenance of body weight and appetite control.
Excitingly, in recent years, researchers have found that these neuroendocrine molecules also play a role in the reward pathway in the brain that is responsible for the pleasurable feelings that you get from your favorite foods. Therefore, the physical and emotional experience of eating may be altered in people suffering from eating disorders.
As Diana mentioned, there was a large emotional component to her disordered eating behaviors. She would binge eat to feel a sense of comfort when experiencing negative emotions and then purge because of the feelings of disgust this behavior elicited. It has been suggested that people with bulimia eat to distract from stress. Anyone who has ever hit the Ben&Jerry’s post-breakup has experienced this. And indeed, the neuroendocrine stress response is hyperactive in many people with eating disorders, which can increase feelings of stress and decrease response to food intake, culminating in overeating. Diana’s high-profile lifestyle and loveless family life likely faded into the background briefly while eating, offering relief, only to reemerge and precipitate purging.
Diana’s openness about her eating disorder famously caused what psychologists and media referred to as the Diana Effect. After going public with her struggles with bulimia, the number of women in the UK receiving treatment for eating disorders doubled. In 1997, clinicians noted that bulimia rates began to decrease, but then began to tick back up after her death that year. We can debate whether there are alternate explanations for this trend, but what’s clear is that Diana’s honesty shined a light on an illness that often keeps its victims in the dark.
Baby Blues
“Then I was unwell with postnatal depression, which no one ever discusses, postnatal depression, you have to read about it afterwards, and that in itself was a bit of a difficult time. You’d wake up in the morning feeling you didn’t want to get out of bed, you felt misunderstood, and just very, very low in yourself.”
As if opening up about her eating disorder wasn’t enough, Princess Diana also got candid about postpartum depression, another taboo mental disorder affecting women. Whether you have children or not, I am sure you can appreciate that childbirth is a stressful experience. You’ve experienced the most intense of biological changes for 9 months and then push the human body to its absolute limit by delivering a baby who will now keep you up at all hours as you fulfill his or her every need. So it’s not surprising that the postpartum period can be a time of increased sensitivity.
However, some women, roughly one in nine according to the Office on Women’s Health, will experience depression-like symptoms for more than two weeks after giving birth. Postpartum depression is more common in women with a history of mood disorders, like Diana. In addition to the classical symptoms of depression that we have covered on the blog, women may experience difficulty connecting with their new babies. In the most extreme cases, they may think about hurting their own child. Sadly, as many as 50% of postpartum depression cases are estimated to go undiagnosed, likely because of stigma or the belief that postpartum mood changes are normal.

The classical hypothesis is that sudden hormone changes after birth drive postpartum depression. This is similar to mood changes seen in premenstrual syndrome (PMS — definitely not me, never heard of it…), except on a much larger scale. In PMS and postpartum depression, estrogen and progesterone levels decline. However, in pregnancy, these hormones are present at concentrations more than 1000 times higher than in the menstrual cycle. Thus, it makes sense that postpartum depression would be PMS on steroids. In fact, researchers have found that giving rodents large amounts of estrogen and progesterone and then rapidly withdrawing them can induce depression-like behaviors, supporting this theory.
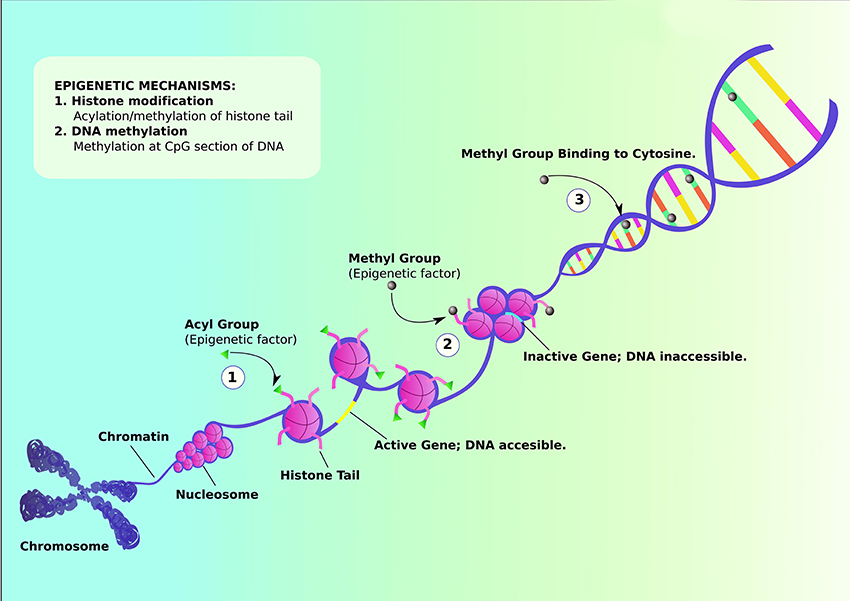
There are many other fascinating areas of research regarding the neurobiology of postpartum depression, like alterations in stress hormones, neurotransmitters, and even the immune system. However, I wanted to share one subfield that I stumbled upon while researching for this post: the role of epigenetics. We’ve talked a lot about the genetics of various diseases. A mutation or variant of a gene causes a change in the protein it codes for, leading to some biological alteration that contributes to disease. This is like changing the text in a document. Epigenetics, on the other hand, affects genes without changing the gene sequence in the DNA. Think of this as font style, size, and bolding, italics, and underlining: alterations to a document that don’t change any of the words on the page.
Epigenetic changes come from the addition of various chemical groups to the DNA. These additions cause the DNA to change shape, or conformation. Some of these conformational changes cause the DNA to loosen, making more room for proteins that promote gene expression to bind. In this case, expression of certain genes in the area of the epigenetic change will increase. Other times, the conformational change causes the DNA to scrunch up, preventing the expression-regulating proteins from binding their targets, and gene expression will decrease. Epigenetics is a fascinating field that is of interest to researchers of pretty much every disease because it bridges the gap between environment and biology, nature and nurture. Environmental exposures can produce epigenetic changes, altering a person’s physiology without altering their DNA sequence.
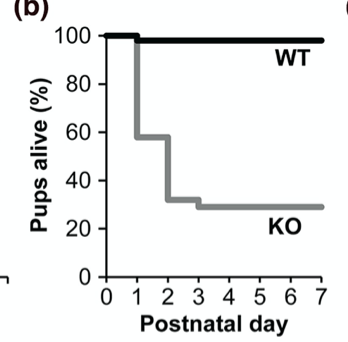
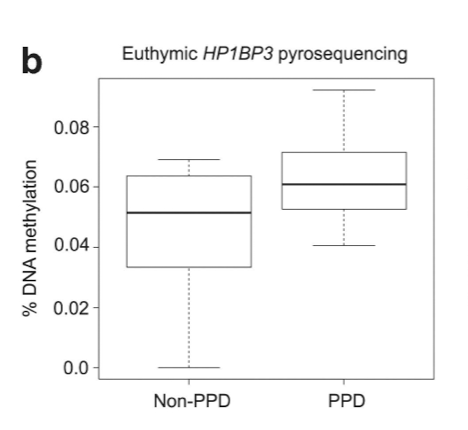
A 2014 study by authors from University of Maryland and Johns Hopkins (shoutout blue jays) studied pregnancy-induced epigenetic changes in women with mood disorders. They identified two genes that were more likely to be silenced by epigenetic changes in women who went on to develop postpartum depression than those who did not. One of these genes, HP1BP3, was previously shown to be involved in maternal behavior. Mice lacking this gene were less likely to go after their pups in a test where they are separated and their pups were less likely to survive. So is the epigenetic silencing of HP1BP3 responsible for defects in parenting behavior in women suffering from postpartum depression? Time will tell! It is likely just one spoke in a complex wheel of physiological mechanisms, but understanding how epigenetic changes contribute to postpartum depression could help identify women who are at-risk so that they can get help before experiencing the same struggles as Diana.
A Cry for Help
“When no one listens to you, or you feel no one’s listening to you, all sorts of things start to happen. For instance you have so much pain inside yourself that you try and hurt yourself on the outside because you want help, but it’s the wrong help you’re asking for. People see it as crying wolf or attention-seeking, and they think because you’re in the media all the time you’ve got enough attention. But I was actually crying out because I wanted to get better in order to go forward and continue my duty and my role as wife, mother, Princess of Wales.”
As Stefanie told you last week, when things got more bleak in Diana and Charles’ marriage, Diana became more desperate. She began to engage in nonsuicidal self injury (NSSI), where someone hurts themselves without intending to commit suicide. Diana described throwing herself down some stairs while pregnant and cutting herself. These are obviously serious actions, but she admitted that she had no intention of trying to take her own life, but rather was “actually crying out”. Studies have found a higher rate of NSSI in patients with eating disorders (around 35-45%), especially those with bulimia, than the general population. One study found that NSSI in eating disorder patients was particularly associated with adverse childhood effects, including traumatic divorces like that of Diana’s parents.
The motivations for engaging in self-harm can vary, but a common reason is because the injury can temporarily relieve persistent negative emotions. This is similar to the explanation Diana gave of her bulimia when she said that purging was like “having a pair of arms around you” for a brief moment. Some imaging studies of people who perform NSSI have found that these patients show increased activation of the amygdala in response to neutral stimuli. The amygdala is a brain region involved in identifying threatening stimuli and triggering the fear responses like fight or flight. Therefore, a popular hypothesis is that NSSI patients have hyperactive fear responses and self injury can somehow blunt this. This could be due to the activation of a separate brain circuit responsible for the internal experience of reward. Researchers found teen girls who engage in self harm experienced an increased sense of “relief” after being exposed to a painful cold stimulus. The subjective report of relief was correlated with brain activity in the striatum, a brain region involved in the reward pathway. This suggests that self injury could be acting as a neurological reward, much like a drug, causing a sensation of relief or improved mood briefly as a result.
Strength in the Weakness
Diana’s own recollections took us through 3 disorders and an array of biological mechanisms, from epigenetics to brain circuitry to endocrine disturbances. Our neuroscientific understanding of bulimia, postpartum depression, and NSSI remains incomplete, and as much as the world knows about Diana, we similarly only understand her partially. Unless she had bravely opened up about her mental health, the world would have been oblivious to her suffering. Outwardly, Diana was vibrant and beautiful and passionately working for people on the fringes of society. Her candor forged a path for talking openly about mental illness and very well may have saved lives by inspiring others to seek treatment. But her mark on mental health isn’t the only legacy she left. Next week, Stefanie will discuss Diana’s long-term impact on the monarchy, and you won’t want to miss it!
If you or someone you know is struggling with depression, self-harm, or suicidal ideation, call the Suicide Prevention Lifeline at 1-800-273-8255.
If you or someone you know is struggling with an eating disorder, contact the National Eating Disorder Association helpline at 800-931-2237.
References
Berner, L. A., Brown, T. A., Lavender, J. M., Lopez, E., Wierenga, C. E., & Kaye, W. H. (2019). Neuroendocrinology of reward in anorexia nervosa and bulimia nervosa: Beyond leptin and ghrelin. Molecular and Cellular Endocrinology,497, 110320. doi:10.1016/j.mce.2018.10.018
Garfinkel, B. P., Arad, S., Neuner, S. M., Netser, S., Wagner, S., Kaczorowski, C. C., . . . Orly, J. (2016). HP1BP3 expression determines maternal behavior and offspring survival. Genes, Brain and Behavior,15(7), 678-688. doi:10.1111/gbb.12312
Guintivano, J., Arad, M., Gould, T. D., Payne, J. L., & Kaminsky, Z. (2014). Antenatal prediction of postpartum depression with blood DNA methylation biomarkers. Comprehensive Psychiatry,55(8). doi:10.1016/j.comppsych.2014.08.017
Jimerson, D. C., Mantzoros, C., Wolfe, B.E, Metzger, E.D. (2000). Decreased Serum Leptin in Bulimia Nervosa. Journal of Clinical Endocrinology & Metabolism, 85(12), 4511-4514. doi:10.1210/jc.85.12.4511
Kaye, W. (2009). Neurobiology of Anorexia and Bulimia Nervosa Purdue Ingestive Behavior Research Center Symposium Influences on Eating and Body Weight over the Lifespan: Children and Adolescents. Physiology & Behavior,94(1), 121-135. doi:10.1016/j.physbeh.2007.11.037
Mendle, J. (2017, August 30). Princess Diana’s Legacy on Mental Health, Eating Disorders. Retrieved from https://time.com/4918729/princess-diana-mental-health-legacy/
Payne, J. L., & Maguire, J. (2019). Pathophysiological mechanisms implicated in postpartum depression. Frontiers in Neuroendocrinology,52, 165-180. doi:10.1016/j.yfrne.2018.12.001
Postpartum depression. (2019, May 14). Retrieved from https://www.womenshealth.gov/mental-health/mental-health-conditions/postpartum-depression
Schreiner, M. W., Klimes-Dougan, B. D., Begnel, E. R., & Cullen, K. U. (2015, September 28). Conceptualizing the neurobiology of non-suicidal self-injury from the perspective of the Research Domain Criteria Project. Retrieved from https://www.sciencedirect.com/science/article/pii/S0149763415002456
The Panorama Interview. (n.d.). Retrieved from https://www.bbc.co.uk/news/special/politics97/diana/panorama.html
Vieira, A. I., Ramalho, S., Brandão, I., Saraiva, J., & Gonçalves, S. (2016). Adversity, emotion regulation, and non-suicidal self-injury in eating disorders. Eating Disorders,24(5), 440-452. doi:10.1080/10640266.2016.1198205
Zhou, Y., & Rui, L. (2013). Leptin signaling and leptin resistance. Frontiers of Medicine,7(2), 207-222. doi:10.1007/s11684-013-0263-5
